R3) Abdominal pain and vaginal bleeding in a patient with reduced pregnancy symptoms
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with abdominal pain and vaginal bleeding.
- Review the DDx considerations in a patient with abdominal pain and vaginal bleeding.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with abdominal pain and vaginal bleeding.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
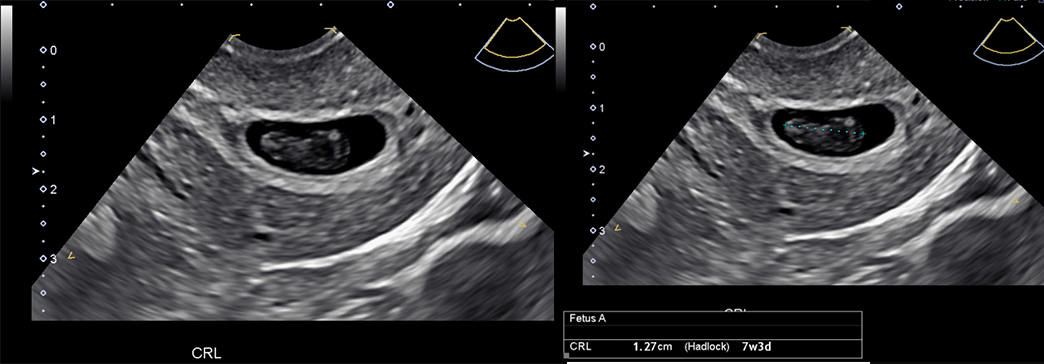
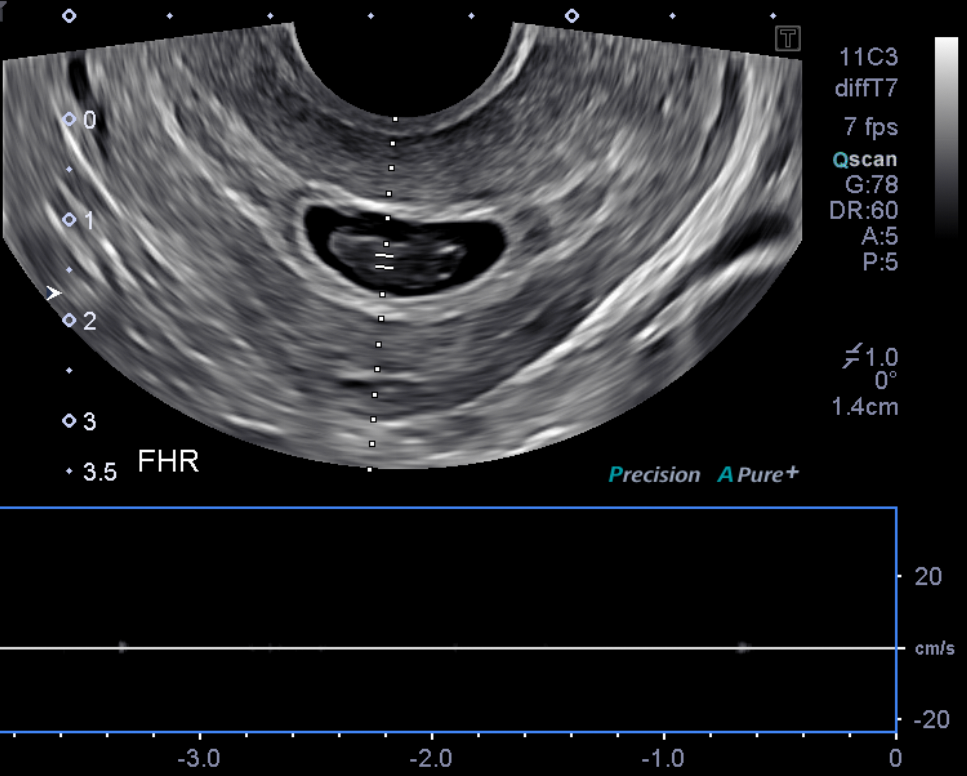
Transvaginal Ultrasound
What best describes the findings on the Crown rump length (CRL) is consistent with a 7-week pregnancy.
The fetal heartbeat is present.

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- There is an increased risk of pregnancy loss during the first trimester. The risk is increased with increasing maternal age and previous miscarriages.
- The diagnosis should be suspected in a patient who presents in the first trimester of pregnancy with vaginal bleeding and abdominal cramping, with reduction of pregnancy symptoms such as breast tenderness and hyperemesis gravidarum.
- A transvaginal ultrasound is the imaging modality of choice to diagnose a nonviable pregnancy.
CRL ≥ 7 mm or mean gestational sac diameter of >25 mm without fetal heartbeat confirms definitive pregnancy loss. If these criteria are not met, follow-up interval imaging should be considered.
Socioeconomic Factors:
- Low income levels are associated with increasing risk of spontaneous abortion.
- Environmental exposure to ionizing radiation, lead, arsenic, and air pollution increases the risk of miscarriage.
- Those with poor access to care or those less likely to expect or recognize a pregnancy (adolescents or perimenopausal patients) may be at higher risk for complications from late presentation.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Seyedeh Mehrsa Sadat Razavi, MS2 - Content Contributor
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator

{kind=link}
{kind=link}